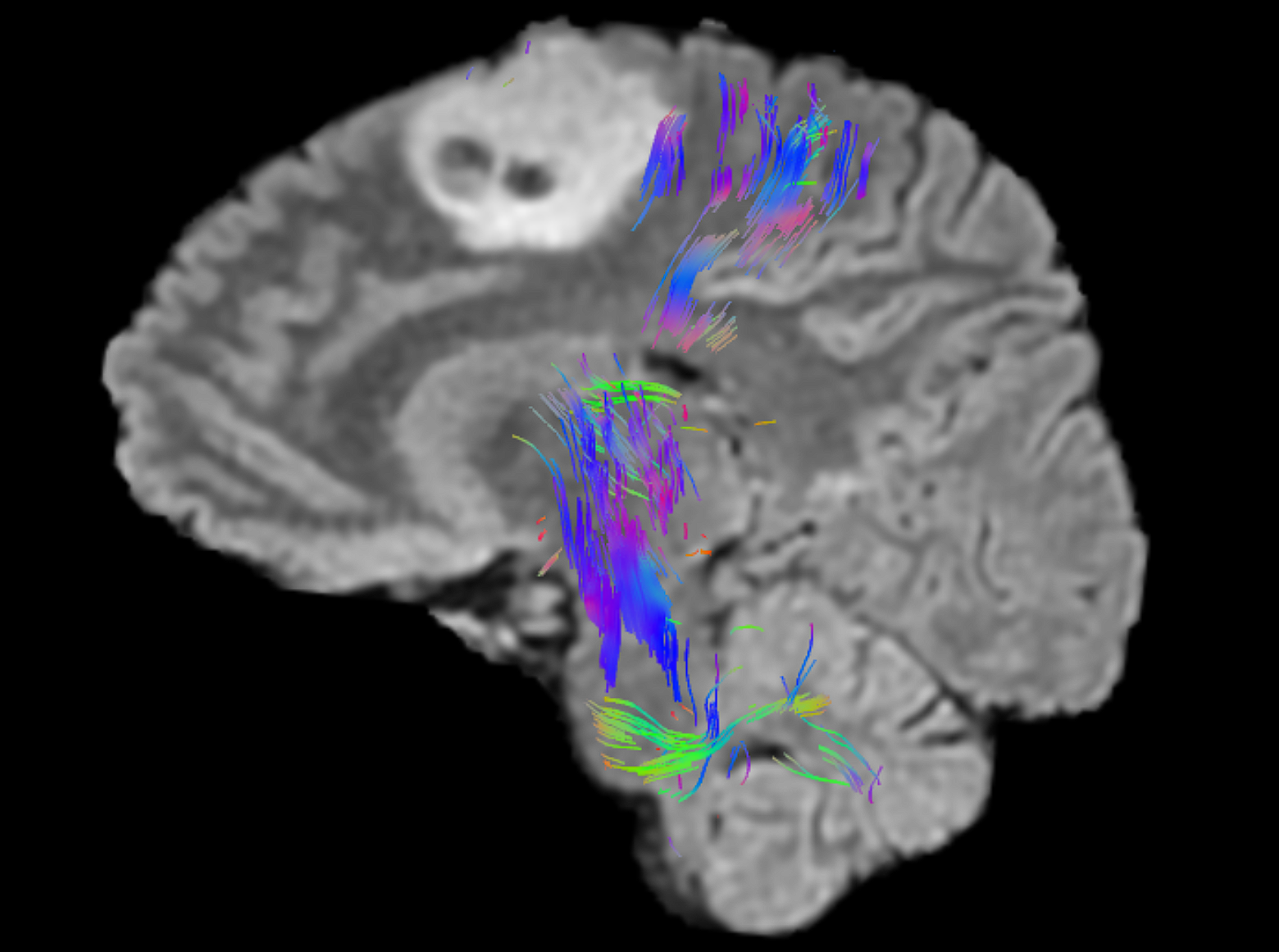
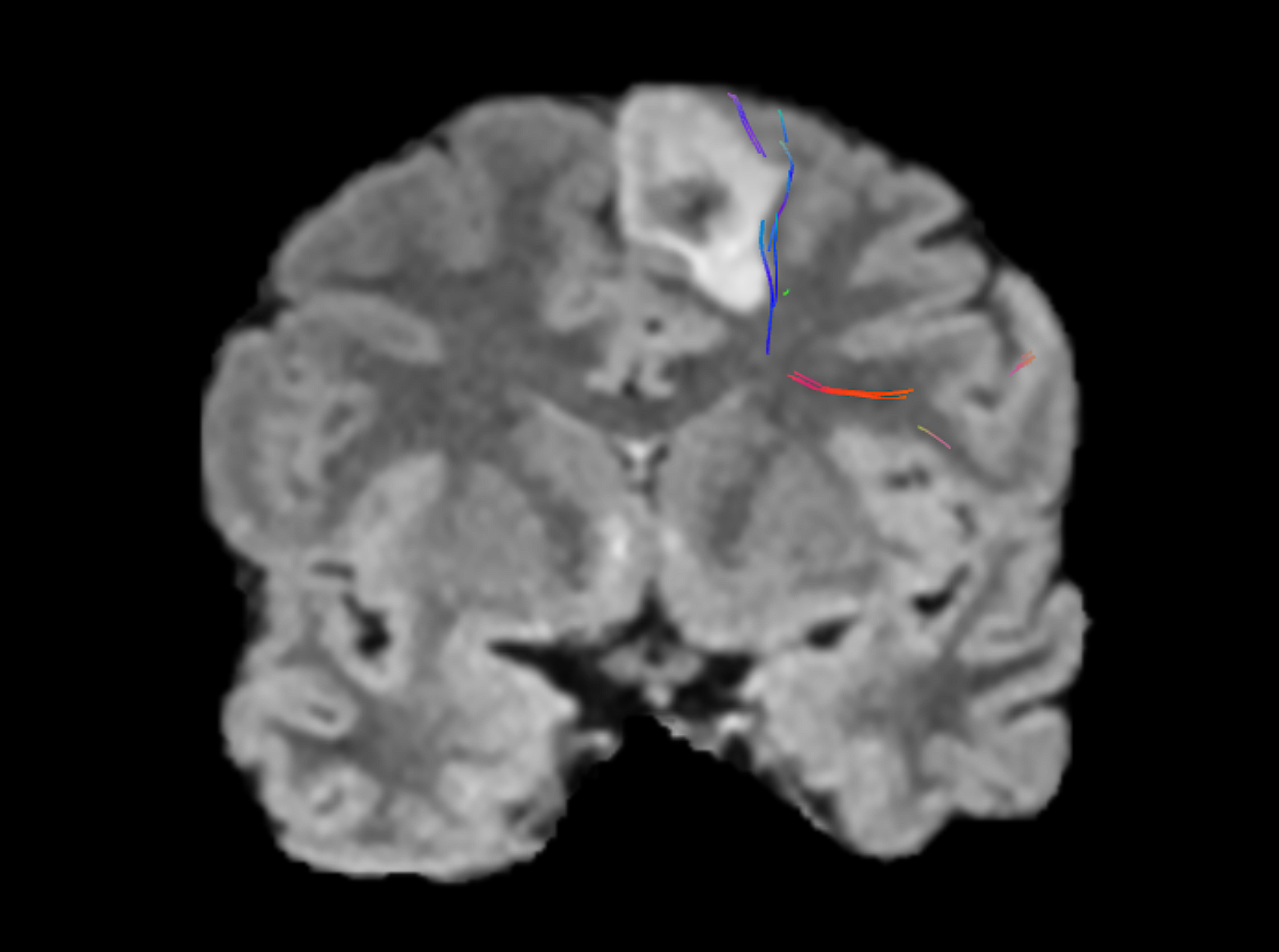
Quicktome was used to evaluate the relationship of the tumor with the surrounding areas, particularly the frontal aslant tract (FAT) in the supplementary motor area (SMA), and the corticospinal tract (CST).
These areas were in close proximity to the tumor and so extra care was needed to avoid damage to the FAT, which can result in speech disorders, as well as impairment of executive functions, visual–motor activities, orofacial movements, inhibitory control, working memory, social community tasks, attention, and music processing. Damage to the CST can lead to an irreversible contralateral motor deficit, and surgical manipulation of the SMA tends to cause transient deficits, recoverable within a few weeks. It is a well-known complication of medial frontal lobe surgery called SMA syndrome.
Performing surgery awake was deemed not possible due to the patient's anesthesiologic contraindications.