Recently, connectomics has been used to explore the heterogeneity of depression. Siddiqi et al identified that independent depressive symptoms and their severity are driven by different connections between the major brain networks which underpin the disorder. Namely, anxiogenic symptoms were driven by connections from the Default Mode Network, whereas dysphoric symptoms - such as sadness and anhedonia - were driven by connections arising from the salience network23.
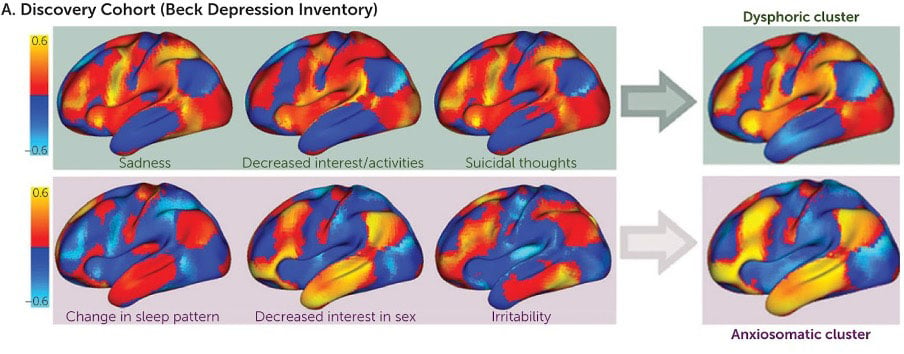
Figure 3. Color map of brain areas responsible for Anxiosomatic vs. Dysphoric symptoms of depression - adapted from Siddiqi et al., 2020
Moreover, evaluating an individual’s unique depression via their own brain connectivity enabled these researchers to adopt a more personalized neurostimulatory approach to effectively treat their patients symptoms. Another study, the Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT), adopted a similar approach, targeting unique brain regions with TMS based on their patients' underlying functional connectivity. This study found that 90.5% of the MDD patients investigated met remission criteria after five days of treatment, demonstrating the time-saving and effective response of leveraging connectomics to treat MDD24.
Connectomics is an exciting tool for studying depression, and it is clear that the human connectome plays an important role in the symptoms which define it. As the field of connectomics continues to progress, future individualized treatments may soon be uncovered.